
The first post in this series introduced the platform terminology of single-homing vs. multihoming. Patients strongly would prefer to have as few portals as possible — ideally one, i.e., a single “home”. However, patients are forced to subscribe to multiple homes since today’s portals are tethered to individual institutions or care providers.
In this post, we’ll introduce the platform terminology of stand-alone vs. network value. Today’s patient portals can provide some stand-alone value, but they provide minimal network value.
In the upcoming third post in the series, we’ll discuss “friction” in today’s portals. In the fourth post, we’ll consider some alternatives; while today’s portals CAN NOT work as configured, we’ll look at some options that could work.
Stand-Alone vs. Network Value
Value is created in different ways for different offerings. Some offerings provide stand-alone value; others provide value through networks and networked data and activities; some provide a combination of these.
Stand-alone value refers to the value provided by an offering that is independent of how the platform is used by others. Network value refers to value created through the activity and usage of others. Network value also refers to network effects or positive feedback loops created through the activities of others.
Let’s use your personal computer as an example to explain the difference between stand-alone vs. network value. Your PC has stand-alone value even when it is not connected to a network such as the internet. You can use a word processing program to create documents. You can create spreadsheets. You can play single-player games such as solitaire.
But…your PC gains network value when connected to the internet or another network. Now, you can share documents with colleagues and collaborate in editing. You can work together on spreadsheets. You can play multi-player games in real-time. You can use your PC to keep in touch with friends and colleagues through email or view information from hundreds of millions of websites,
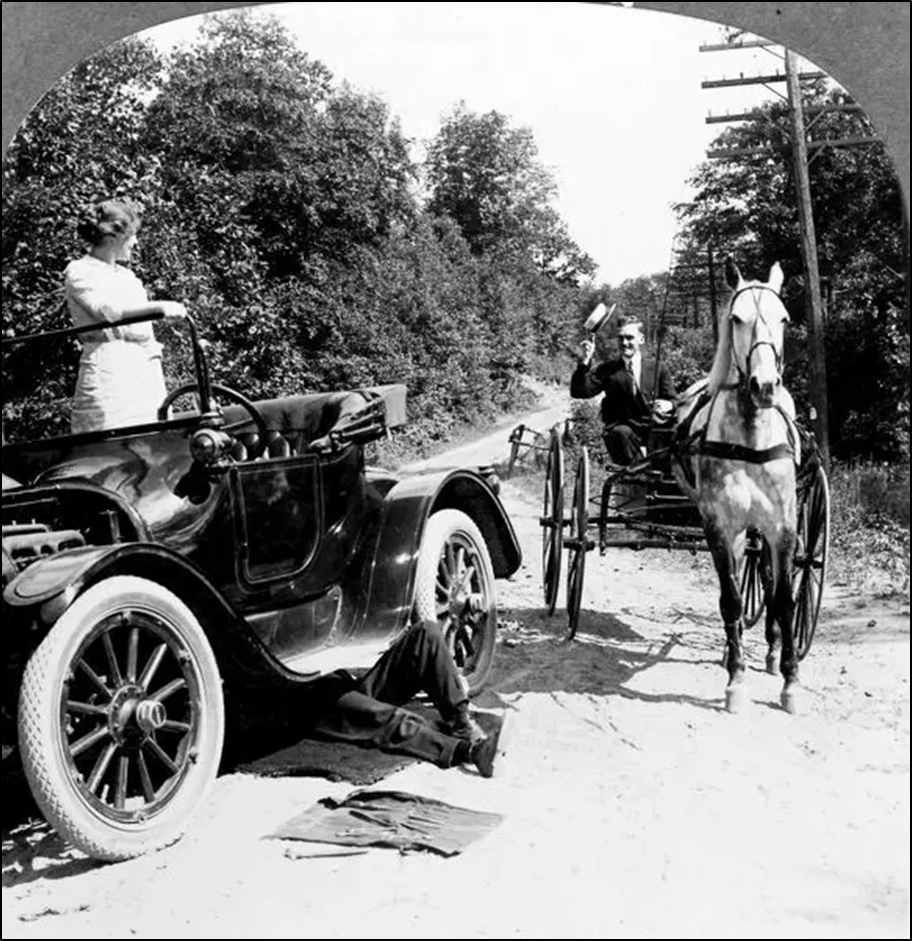
Consider another example — automobiles. When invented over a hundred years ago, cars provided stand-alone value when driven on gravel roads originally designed for a horse and buggy.
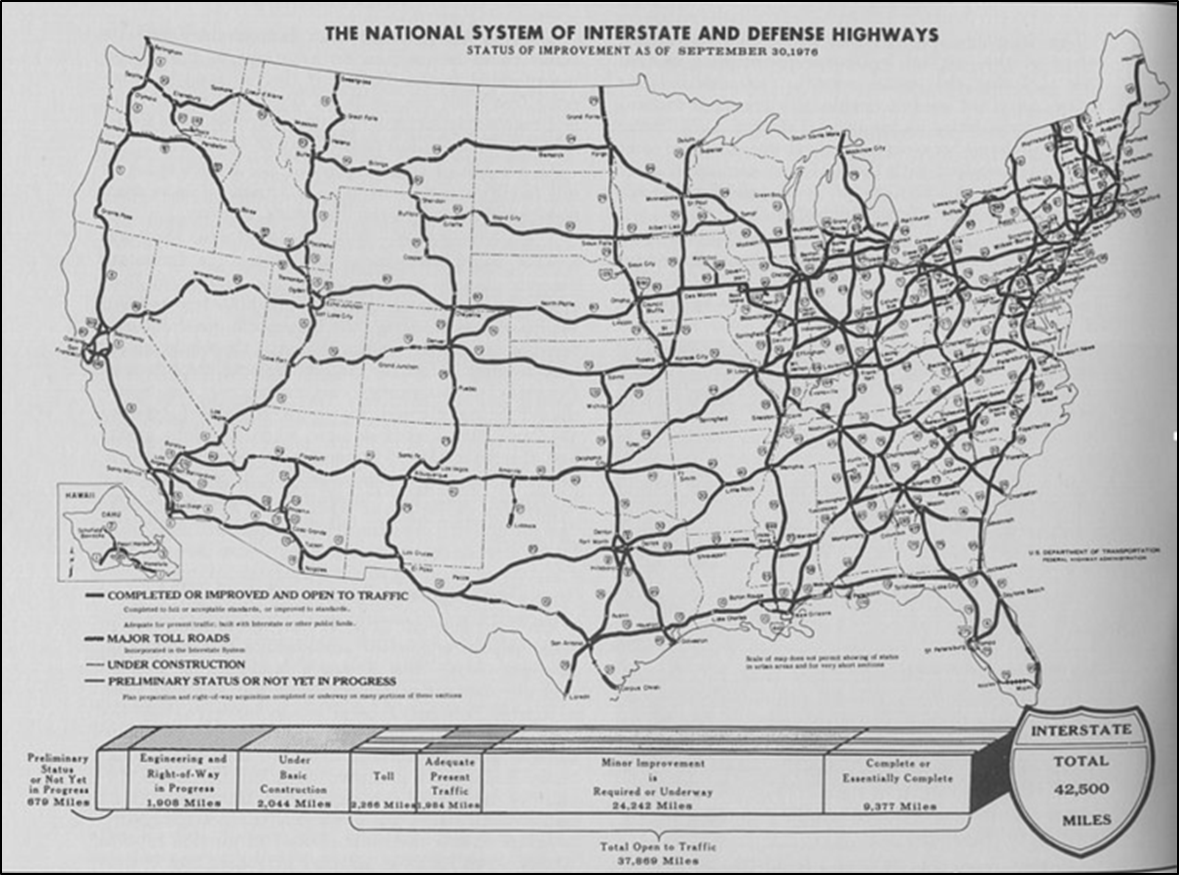
A new level of value was added to cars in the 1950s through the creation of the Interstate Highway Network.
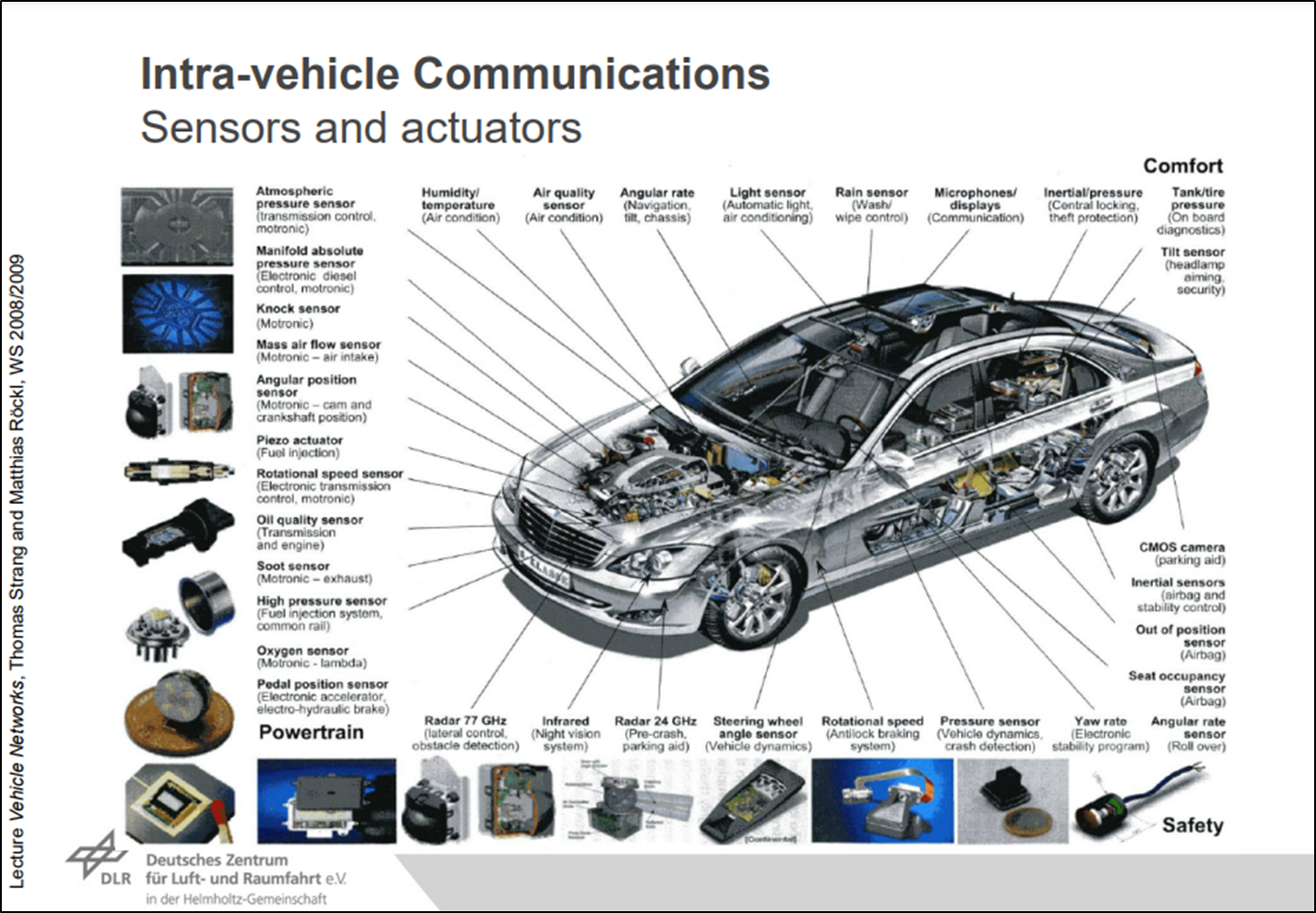
Today’s cars are increasingly intelligent — they gather and share multiple types of data to improve individual and collective vehicle performance and safety.
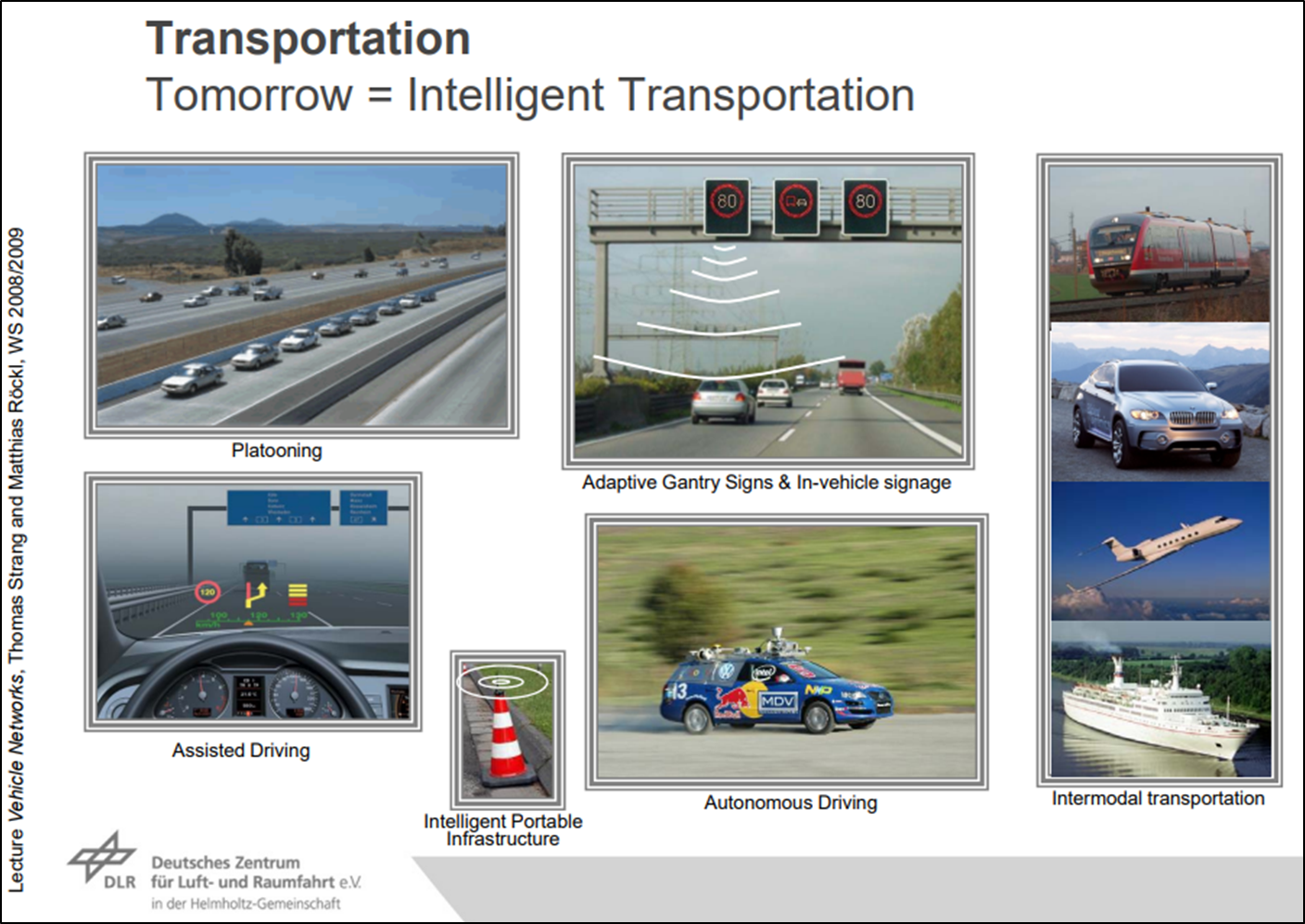
The automobiles of tomorrow promise to deliver even more value as they increasingly join networked, intelligent transportation systems.
There’s a pattern here worth noting. While products or services often initially provide primarily stand-alone value, over time they have great potential to gain network value.
“Come for the tool, stay for the network”
Andreesen Horowitz partner Chris Dixon coined the phrase: “come for the tool, stay for the network”.
The idea is to initially attract users with a single-player tool and then, over time, get them to participate in a network. The tool helps get to initial critical mass. The network creates long-term value for users and defensibility for the company.
Platform expert Sangeet Choudary described how OpenTable’s business model is an example of “come for the tool, stay for the network”:
Service booking systems like OpenTable (restaurant reservation) work in a similar manner. To seed usage among one side of the network (restaurants), the company distributes booking management systems that the restaurant can use as standalone software. Once OpenTable had enough restaurants on board, and hence access to their seating inventory as well, they opened out the consumer side to allow them to start making bookings and collecting a lead generation fee from the restaurants.
As we will discuss below, today’s patient portals can provide some “tools”, but there’s no clear route to creating and capturing value across a network of care providers.
Today’s Patient Portals Offer Stand-Alone Value
Today’s patient portals do offer some value to some people.
Portals offer mostly the ability to conduct discrete transactions within one provider organization, e.g, to pay bills, to check on a lab result, to request a prescription.
Today’s portals also can work for patients in extremely narrow provider networks, e.g, in an organization such as Kaiser Permanente.
However, most patients see a wide range of providers. A study in the International Journal of Medical Informatics found that:
- Only 5% of Medicare patients have records with only 1 vendor
- 20% have medical records w/ 8+ vendors
But, Today’s Patient Portals Miss Out on Network Value
Software Advice provided a list of patients’ most desired features in today’s portals:
- Scheduling appointments online
- Viewing health information (e.g., lab results or clinical notes)
- Viewing bills/making payments
- Checking prescription refills/requests
- Filling out pre-visit forms (e.g., intake form)
- Sending messages to my care (healthcare provider) team
- Updating medical history
As you glance at the list, you should note that features in today’s patient portals almost exclusively provide stand-alone value — NOT network value. That’s because they are tethered to single institutions or care providers.
Let’s take this a step further. Consider some examples of network value that CAN NOT easily be provided by today’s patient portals:
- Creating and implementing one care plan across a patient’s team of care providers
- Seamlessly sharing patient data
- Care coordination across providers
- Analytics across providers
- Population health management
Chronic disease management is a case study illustrating how today’s portals fail. A diabetic patient could have an extended care team — a primary care physician, an endocrinologist, nurses, a diabetic educator, a podiatrist, an optometrist, a social worker, a nutritionist, and more. What if each of these has their own portal? #FAIL
Chronic disease accounts for 86% of health care costs. Today’s portals offer little help in improving quality or reducing costs.
The inability of patient portals to provide significant network value inhibits achieving critical mass and network effects. It also limits interest by potential 3rd party developers.
This lack of network value explains much of the tepid adoption of patient portals documented in the first post of this series. Referring back to Chris Dixon’s explanation above, patients can come for the tools…but there’s no network to stay for.
Series: Why Today’s Patient Portals CAN NOT Work:
- (Part 1) Platform Terminology Explains Why Today’s Patient Portals CAN NOT Work
- (Part 2) Today’s Patient Portals CAN NOT Work: An Inability to Capture Network Value
- (Part 3) Today’s Patient Portals CAN NOT Work: Friction ACROSS Portals
- (Part 4) The Missing Ingredient in Today’s Patient Portals: Network Effects
This post was originally published in The Healthcare Platform Blog. It is republished by Open Health News under the terms of the Creative Commons Attribution-Share Alike 3.0 Unported License (CC BY-SA 3.0). The original copy of the article can be found here.